Transitioning to SLS

The ability to obtain and sustain single limb stance (SLS) is a foundational movement pattern. It is necessary for the following activities:
- Walking: every step contains a portion of time when SLS is obtained
- Step Management: the process of step ascent/descent involves being in SLS
- Curb Management: to get up or down a curb, transitioning to SLS is needed
- Obstacle management: to avoid collision with obstacles on the ground
- Reactionary Balance/Stepping Strategies: to make the action of stepping to catch oneself, the weight must be first unloaded and this occurs through a transition to SLS on the non-moving limb
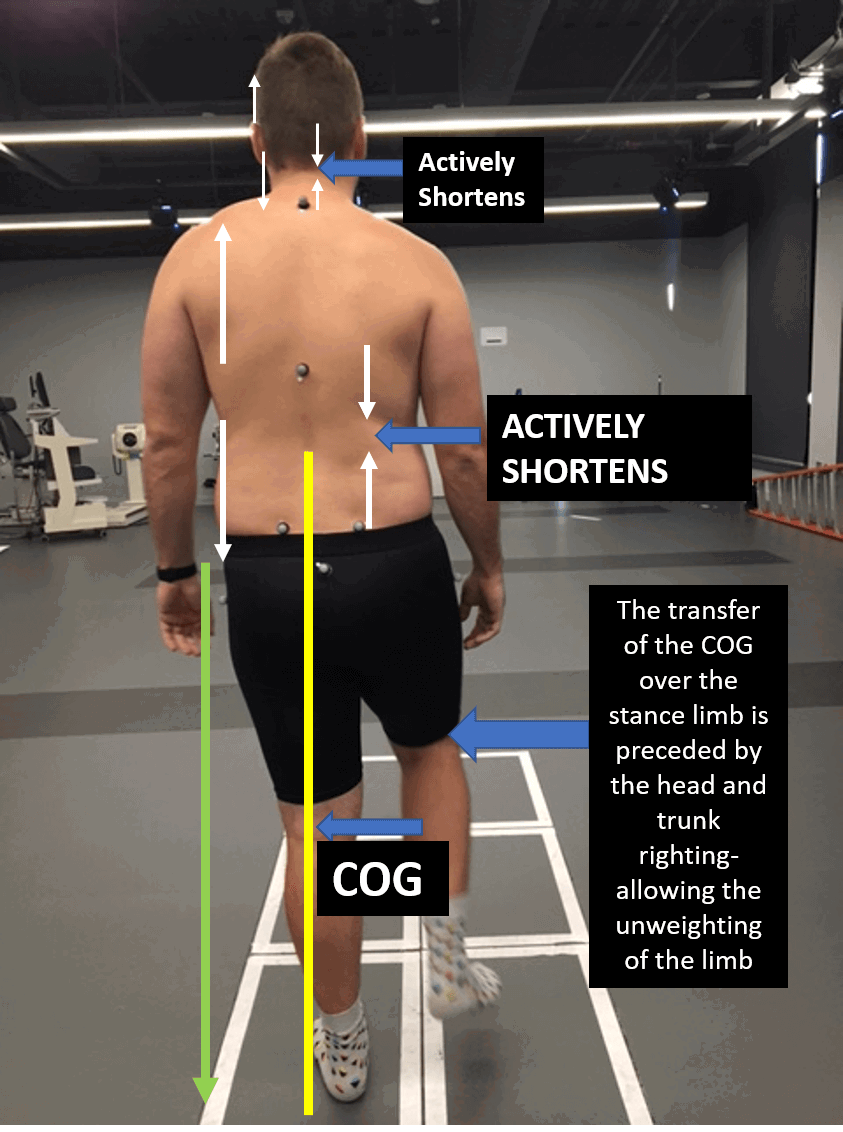
NORMAL MOVEMENT PATTERN
The transition is initiated from the proximal muscles where the trunk, in the frontal plane, assumes a shortened-lengthened asymmetrical firing pattern which provides the basis for the proximal stability needed for the unweighted limb to intentionally be moved (for walking, stepping, obstacle negotiation, stepping strategy)
NORMAL:
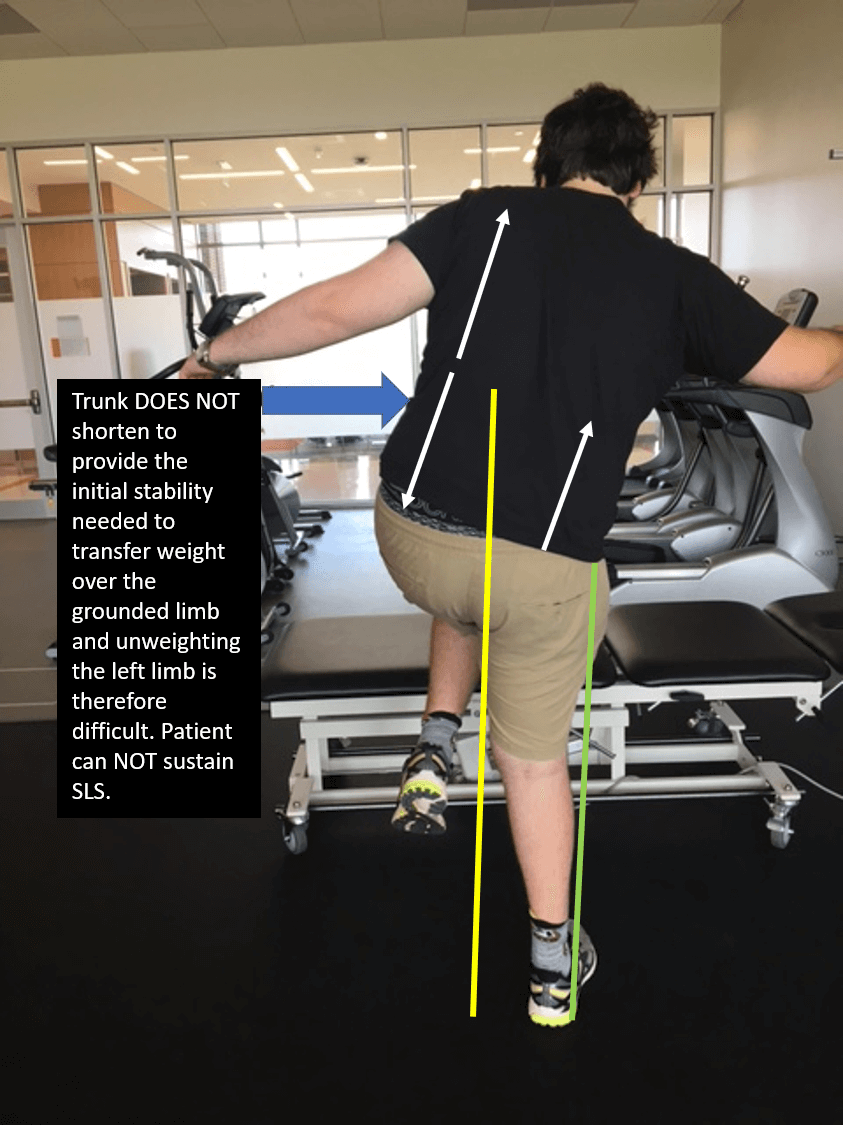
In contrast, this individual uses a compensated pattern to attempt to achieve SLS:
MOST LIKELY IMPAIRMENTS CONTRIBUTING TO THIS COMPENSATION:
The most likely reason someone would choose this pattern for achieving SLS are as follows:
- Lack of glut med activation on RIGHT HIP
- Lack of frontal plane lateral trunk muscle shortening on the LEFT side
- Lack of frontal plane lateral cervical shortening on the LEFT side
In this case, the patient has had a traumatic brain injury and his LEFT side is his weaker side. In fact, his glut med on BOTH sides, via dynamometry, is normal. Therefore, the most likely reason for this appearance is the lack of automatic activation on the LEFT side of the trunk to provide the condition for stability for the successful weight transfer. Therefore, this supports the fact that SWING PHASE (unweighting of the limb) is often difficult for patients NOT because the hip flexors are weak (remember, only 2+ MMT for normal swing) but because the TRUNK MUSCLES on the same side of the swing limb (left) need to be capable of providing the necessary activation for trunk shortening for the stability needed for SLS and swing.
NORMAL PATTERN WHEN ACCESS TO THE CORRECT
MOTOR RECRUITMENT IS AVAILABLE
 Notice the difference in strategy when the STRONGER right side lateral trunk muscles do what is needed to allow for the weight transfer to SLS to the weaker (left) side. So in this circumstance, he is BETTER at SLS on his weaker left side because the demand to achieve this is high on the STRONG SIDE RIGHT TRUNK muscles.
Notice the difference in strategy when the STRONGER right side lateral trunk muscles do what is needed to allow for the weight transfer to SLS to the weaker (left) side. So in this circumstance, he is BETTER at SLS on his weaker left side because the demand to achieve this is high on the STRONG SIDE RIGHT TRUNK muscles.
RULE:
Right Weight Shift: Left side trunk shortening
Left Weight Shift: Right side trunk shortening
Allows the COG to shift toward the SLS side.
HOW TO FACILITATE SLS:
ASSESSMENT OF SLS ABILITY:
As with the other tasks, we don't want to just do it for the patient, but we want to ask them first to do it. This gives us an opportunity to feel and see the strategy they use to accomplish this task.
Then, we hypothesize what the limiting factor is and then give to them the missing piece (more glut med control, appropriate length/shortening of lateral trunk muscles or cervical muscles) and repeat the task and see if there is a difference.
In the case below, when he attempted it, he demonstrated the compensation as you see below:
I had already assessed his hip muscles and knew that the glut med was as strong as the other side and did not think that was a contributing factor. My hypothesis was that it was a trunk issue and that if he appropriately shortened the left side with resultant lengthening on the right side, he would have a more successful weight transfer and could sustain SLS more successfully. So, I have to assess this. I had him raise his right hand up high which, mechanically, imposes a demand to shorten on the left and lengthens the right. Look at the difference in pelvic position, COG and stability. For this young man, it was a trunk issue.
*Functionally, he tripped a lot because he could not clear his left (weaker) leg, not because the leg was too weak to lift and clear the ground/curbs, etc, but because the trunk did not do its job to initiate the stability needed proximally for the dynamic weight shift that preceded unweighting of a limb for swing, clearance, curbs or step management.

PATIENT WITH NEED FOR MORE ASSISTANCE/SAFETY ISSUES:
Below is a video that shows a key method of performing Sit- Stand as well as standing assessment and transitioning to SLS when you do not have a second person and perhaps the patient is larger than you or needs maximal assistance.
This is a great method for assessment as well as a spot for interventions. The END POINT (solid surface) always goes on the GOOD SIDE.